|
Henry R. Vaillancourt MD MPH FAAFP
|
|
In New England we are fortunate to experience four distinct seasons- however, each one has its good and bad sides. One that we often think of as the least enjoyable is winter. In this “blog’, I’d like to share with you some common-sense tips for enduring the cold weather and preventing your succumbing to a winter weather malady. The first thing to bear in mind is how our bodies lose heat. The same mechanisms that help us to endure very hot summer weather can be our undoing in very cold winter weather. The first one is radiation of heat; this occurs when surfaces surrounding us are cooler and heat energy leaves our bodies. The second is conduction which occurs by heat loss through direct contact with a surface that is cooler than we are. The third is convection which occurs when moving air carries heat away from the body’s surface. The final one is evaporation which occurs when water is lost from the skin (sweat) causing body heat to be lost during this process. In cold weather, radiation and convection are the two main ways that we lose heat. Sweating, occurring during heavy exertion, can also be a significant issue in so far the sweat does not evaporate, but remains on the skin and becomes a very efficient conductor of heat away from the body- as well as being able to be frozen. Unless you are sitting for a prolonged period on a cold surface, conduction is much less of an issue. The three significant cold weather dangers are frostbite, hypothermia and carbon monoxide (CO) poisoning. All three can be life-threatening and the last two can be fatal. In this blog, I will discuss frostbite and hypothermia, and in a later one, CO poisoning and how easily it can occur . Frostbite is an injury to the body that is caused by an actual freezing of body tissues. The parts of the body most at risk for frostbite are the ears, nose, cheeks, chin as well as toes and fingers. In fact, any part of the body that is in prolonged contact with a cold surface (remember conduction) can also be affected. As a result of this condition, a person can suffer permanent injury. In cases that are severe, a person may even end up with an amputation of the affected part. Those people at greatest risk for not only frostbite, but hypothermia are the elderly, the very young, anyone who may have a condition associated with “poor circulation”, and people (or pets) outdoors for prolonged periods. Of, course, those who don’t dress properly in very cold weather are also at risk. Sorry, but wearing shorts or light shoes in very cold January or February weather is like dipping your toes in a piranha tank- you’re asking for trouble! Many people ignore the early signs of frostbite which can be a redness of the skin, and a tingling or a burning sensation. These may indicate that frostbite is beginning and if one doesn’t get out of the cold, it may progress. If no action is taken, the skin may begin to appear white to a slight yellow in color, numbness may set in, and the skin may then take on a waxy to firm character. In some cases, because of the numbness, a person is not aware until someone else points out the color changes! Unfortunately, as skin tissues freeze, they become numb and less sensitive. In the early stages of frostbite, getting out of the cold and into a warm room is the first step. The affected body part can be warmed gently- usually by immersing in warm water. Note that I say “warm”, not “hot”. A good rule of thumb is that anything that is not comfortable for an uninjured body part is not appropriate for a potentially injured body part! Another way to gently warm an area is by body heat -in other words, against the body such as in the armpit, between warm hands, etc. If there is already numbness or skin texture changes, then one is going to need medical attention. A person should never walk on toes or feet that are frostbitten, since more damage can be done to the already injured tissues. Other mistakes are massaging a frostbitten area ( since vigorous rubbing of injured tissues may increase swelling and damage), or the “Old Wife’s Tale” of rubbing it with snow. Because a frostbitten area can be numb, you should never warm it by the heat of a stove, fireplace or against a radiator. There is the likelihood that an early cold injury can be converted to a heat injury! Remember, however, that if there is the suspicion that frostbite has occurred, you need to seek medical attention, and only use the above methods if immediate medical attention is not available and until you can get it! Hypothermia is a condition where one develops an abnormally low body temperature. This is the result of having reached a point where your body’s production of heat is surpassed by its loss of heat. The problem with this situation is that the brain is sensitive to low body temperatures and it begins to function less effectively. In fact, its metabolism slows down. That is why in some medical situations a medically-induced state of hypothermia may be used to protect the brain. Usually, when hypothermia sets in, a person’s judgment may be sufficiently impaired so that they don’t know what is happening. Fortunately, there are warning signs of hypothermia, but they can quickly pass. In adults, shivering, particularly when intense and prolonged, should never be ignored. When we shiver, we rapidly contract muscles as a way to produce additional heat. However, this is a metabolically intense action that cannot be sustained for long. As time progresses –which can be very short in extreme conditions- confusion starts to set in. Along with this may be clumsiness, then slurring of the speech, and trouble thinking. Drowsiness is a dangerous sign. In young children, particularly infants, their skin may take on a bright red color yet it may feel very cool to the touch. They may also seem sluggish and difficult to arouse. Who is most at risk of hypothermia? Clearly, anyone remaining outdoors for extended periods of time is at risk. This can include those working outdoors as well as people participating in recreational activities outdoors. Hypothermia can occur at both very cold temperatures and even cool temperatures- such as above 40 degrees! Remember, convection (strong winds), radiational loss and conduction (through cold surfaces or cold water) are the major factors. The elderly are at particular risk of hypothermia; even at “ just slightly cooler” temperatures. This is because they often have little body fat;their skin is thinner and more conductive; they may have other underlying medical conditions; or they may be taking certain medications that place them at risk. In situations where one may not have adequate indoor heat and poor nutrition, the threshold for hypothermia is even lower. It is always a good idea to check on your elderly relatives and neighbors when the weather is very cold, since few people can say or even realize they are becoming hypothermic. Infants, for many of the same reasons, are also at risk. Drinking alcohol can also increase one’s risk for hypothermia. Alcohol does not warm a person; in fact, it increases heat loss from the body. The image of a St. Bernard dog with a keg of brandy around its neck is one that needs to be forgotten! Alcohol dilates blood vessels. As the precious warmth leaves our bodies, we may experience a feeling of warmness on our skin, but we are making things worse. The warm feeling in our stomachs is due to the mild irritation of the alcohol, but in no way does it increase our body heat. Because hypothermia can be a life-threatening condition, medical attention is necessary. In very mild cases, or until medical evaluation is available, there are some measures that can be taken. The person should be brought into a warm room. Wet clothing needs to be removed. If possible, any type of warm beverage- other than an alcoholic- one can be given. Warming the person with an electric blanket, body contact or gentle heat are useful. Since the center of our body is the area most in need of heat, it should be warmed first- which is why warm beverages are good. Because the number and types of medications that can increase one’s risk for hypothermia is large, it is much better to ask your pharmacist. The next time you get your refills, if any of your medications do place you at risk.
0 Comments
This blog is being devoted to one question- “What is the most effective way to treat the nasal symptoms of a cold”? I am addressing this as a result of a recent medical journal article. For most people with the “common cold”, it is the runny, congested, sneezing nose that causes us the most discomfort, so this seems appropriate. However, before this can be addressed, two questions need to be answered: 1. What is evidence-based medicine, and 2. What is the Cochrane Library of systematic reviews? In a nutshell, evidence-based medicine utilizes the results from well-designed and well-analyzed studies, along with clinical expertise to guide the treatment of a patient. A specific question is formulated, and the results of numerous studies are typically evaluated by a panel of experts and clinicians and then aggregated to answer it. As part of the conclusion, the strength of the information is evaluated, very often ranging from low quality to high quality evidence or degrees of risk versus benefit. This approach (which I have highly simplified) is then applied to determining the best intervention or treatment for a patient or a condition. Very often, these numerous queries are grouped into databases. One well-known database is the Cochrane Libraries. Their researches have looked at thousands of clinical questions and then scoured the literature for the best evidence-based answers. That being said, this past October, the British Medical Journal, a prestigious and well-reviewed source of information, published an article (BMJ 2018;363:k3786) entitled, What treatments are effective for common cold in adults and children? (I would recommend that everyone look up the article, as they have a great graphic that explains everything I am about to summarize.) The authors searched the Cochrane libraries, other databases and specific articles that were not found in these collections and from this investigation, classified most of the known interventions for nasal symptoms into four areas: 1. Small or possible beneficial effect 2. No or unclear effect 3. Likely to be harmful 4. No evidence of effect. In doing so, they addressed the 3 most common nasal symptoms- congestion, runny nose and sneezing when evaluating treatments. In the first category, “Small or possible beneficial effect”, they concluded that the combination of an analgesic plus decongestant spray possibly had an effect on the severity of congestion (low quality of evidence), but no effect on runny nose or sneezing, and there was an increased risk of side effects (moderate quality evidence) from a decongestant; such as nervousness, insomnia, palpitations, etc. The combination of an antihistamine, decongestant spray and analgesic possibly had a benefit on congestion, runny nose (low quality of evidence) but no effect on sneezing and may place one at risk for adverse events such as sedation, insomnia, palpitations, etc. A pure decongestant spray, alone, had a small effect on congestion (low quality of evidence), but none on runny nose or sneezing and if used properly no increased risk of an adverse event. Anti-inflammatories (ibuprofen, naproxen, etc.) had only a small effect of the severity of sneezing, but none on any of the other symptoms. Antihistamines, alone, had no effect on severity of congestion, a small effect on severity of a runny nose and a small effect on sneezing, but for all 3 symptoms the effect on how long the symptoms lasted of them was unclear; in other words, do they shorten their duration? The next category was “No or unclear effect”. An antihistamine plus an analgesic showed there was an unclear effect on reducing the severity of congestion or sneezing and no data regarding effects upon a runny nose. Using just an analgesic alone such as acetaminophen had no effects on any of the 3 nasal symptoms. Using a non-sedating antihistamine alone had an unclear effect on the severity of nasal congestion and no effects on a runny nose or sneezing. African geranium extract also known as Pelargonium sidoides (becoming popular) had an unclear effect on congestion and there was no data or studies that looked at its effects on a runny nose or sneezing. Salt water nose irrigation yielded the same conclusions- possibly no effect on congestion, and no data regarding its effects on sneezing or running of the nose. Under “Likely to be harmful”, were antibiotics. As we have told our patients on numerous occasions, antibiotics do nothing for the common cold. In some situations, they may be used to prevent a complication in someone so prone; however, this should be discussed with your healthcare provider. Under the last category, “No evidence of effect” on nasal symptoms of congestion, runny nose and sneezing were: antivirals, Chinese medicinal herbs, Echinacea, Eucalyptus oil, increased fluid intake, garlic, ginseng, heated humidified air, honey, probiotics, vapor rubs, Vitamin C and zinc. With almost all of these substance there was no data to support their efficacy on reducing any of the nasal symptoms associated with the common cold. So, what can we conclude from this exhaustive review? The first is that they were looking at nasal symptoms, and not necessarily cough, body aches or sore throat. It is always a fine line as to whether to treat a symptom and cause an adverse effect or “grin and bear it. Coughing is a sign of irritation to the respiratory tract, and nature’s way of clearing it of debris or invaders. An irritative, dry cough is a significant nuisance that not only can keep you awake, but further spread your virus to those around you. If you are going to use something for coughing, it is always best to use a single substance medication rather than a combination of ingredients some of which you most likely don’t need. In this case, over the counter dextromethorphan would be a good choice. But, be aware of a potential interaction between certain antidepressants and this medication. Ask your healthcare provider or pharmacist first. Most non-Streptococcal (non-Strept) sore throats can be treated with salt water gargles, lozenges and agents that soothe and prevent dryness. Unless the Streptococcal test or culture is positive, there is little role for antibiotics in treating this symptom. A fever is the body’s response to an infection and may play a role in stimulating immune cell functions and delaying viral reproduction. A low-grade fever with a cold may not need treatment. Significant body aches or headaches might. It is beyond the scope of this blog to discuss when or why a fever may need to be treated; speak to your healthcare provider So, in summary, “What works best for nasal symptoms?” Whatever does the least harm, is used for the shortest amount of time, and is understood by you that it may do little. Please be aware that nasal decongestant sprays, if used for more than 3 days or more frequently than the directions indicate, can lead to significant rebound congestion and problems. As far as dealing with a cold, in general, the tried and true advice still pertains: get rest, drink plenty of fluids, and take measures to prevent spreading it to others (wash your hands, cover your mouth when coughing or sneezing, and stay home). But foremost of all, when in doubt as to what to do, call your healthcare provider! Even though we have just gotten over a heat wave and still expect more warm weather to come, it’s that time of the year where flu shots become available, and getting one “sooner than later” is often recommended (especially for our older population). I’d like to summarize some recent scientific/medical papers that have presented new data about Influenza A & B, as well as flu shot efficacy and timing.
The first series of articles deals with shedding of Influenza viruses by infected people:
This year’s flu season, according to the CDC, was marked by an overall limited protection from the flu shot. This was due to the fact that the H3N2 strain (a Type A Influenza virus) was the dominant one. It accounted for 58% of all Influenza virus subtypes, and there was not a match with the flu shot given. This resulted in an overall efficacy against the A subtypes of only 30%. Although the match for type B influenza viruses was good, they only accounted for 31% of the circulating virus subtypes. Consequently, the overall efficacy for the vaccine this past season was only 38% (adjusted for all ages). Nonetheless, the CDC stated the vaccine likely prevented upwards of 90,000 hospitalizations due to the flu (CIDRAP News, July 02,2019, http://www.cidrap.umn.edu/news-perspective/2019/07/poor-late-season-protection-limited-flu-vaccine-impact-2018-19). Looking at other CDC data for the period October 1, 2018-March 30,2019 (https://www.cdc.gov/flu/about/burden/preliminary-in-season-estimates.htm), there were approximately 38 million cases of influenza, nearly 18 million flu-related medical visits, upwards of 549,000 hospitalizations due to the flu, and upwards of ~51,000 flu-related deaths. A series of articles looked at how effective the flu shot is:
So, what do we conclude from all of these articles? Flu shots significantly reduce the risk for influenza-related hospitalizations and complications, getting yearly flu shots also reduces risk for a severe infection (independent of efficacy of the vaccine), high dose is more effective that standard-dose shots in the elderly, protection from the flu (efficacy) wanes as the season progresses, and delaying the flu shot until the late fall may make sense (but there are risks that “flu season” could begin earlier than expected). The final message is- get your flu shot, there is no reason not to!!! This posting will serve as a prelude to a more detailed discussion of tick-borne diseases. The infographic is courtesy of the CDC and may serve as a discussion basis for you and your healthcare provider should you have a tick attached. 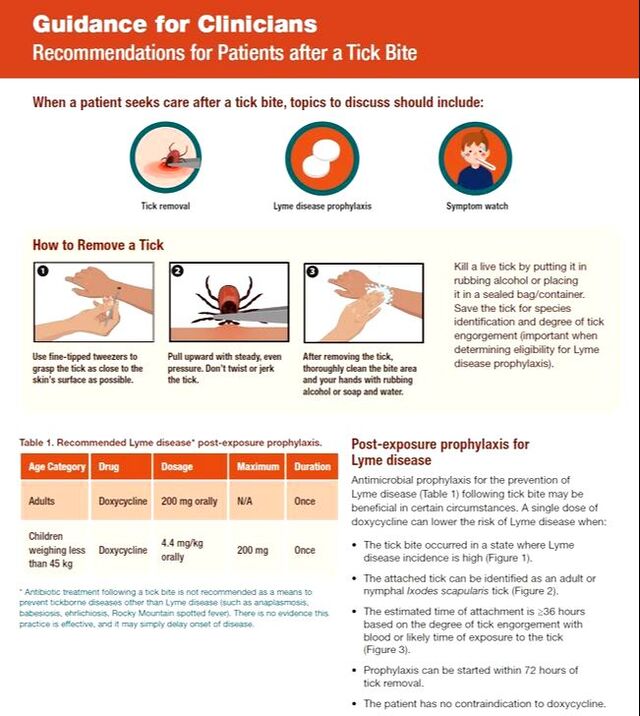 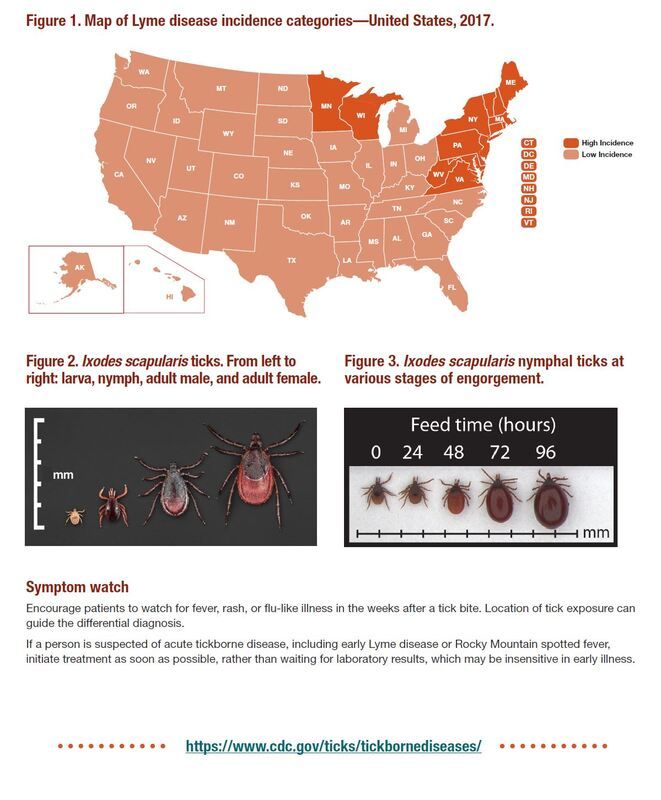 A study just published in the April 17th issue of Nature (Vol. 568, pages 336-343, Restoration of Brain Circulation and Cellular Functions Hours Post-mortem) raises a number of interesting ethical and scientific questions. In a short summary, the study used a system called BrainEx that perfused brains removed from pigs that had been killed up to four hours earlier. The solution used contained a host of nutrients and chemicals that promotes recovery from lack of oxygen. This enabled them to restore some functional activity as well as allow preservation of structural activity four hours after “death”. In other words, a dead pig’s brain began to show biochemical and electrical signs of functioning at a cellular level, but no EEG signs associated with what we consider to be “consciousness”.
Traditionally, we have considered 4-6 minutes without oxygen as being the upper limit of time before irreversible brain injury and death occurs. In this study, pigs’ brains (removed from their skulls) were “revived” after four hours. The authors conclude that “under appropriate conditions the isolated, intact large mammalian brain possess an underappreciated capacity for restoration of microcirculation and molecular and cellular activity after a prolonged post-mortem interval”. What are some of the questions raised? First of all, are we being too quick to assume that a brain has been irreversibly damaged after circulation has stopped? Although the pigs’ brains did not show any EEG activity, could this have recurred if they had continued with the perfusion for a much longer time than they did in their study? Although they used pig brains, we need to realize that pigs are more closely related to us, both immunologically and structurally, than we give credit for. Bear in mind, that pig valves were commonly used in human hearts, and other tissues are being considered in xenotransplantation (I suggest you read about this subject, further, since some of the work being done is fascinating). Are these findings going to be applicable to the human brain? The implications for when to consider someone “dead” and an organ donor have already arisen as a result of these preliminary findings. This was touched upon in a “Comment” to the study, entitled “Pig experiment challenges assumptions around brain damage in people”, in the same issue. Clearly, this study needs to be replicated and the evolution from research to clinical application is a very long way off. The input of a number of specialists ranging from medical ethicists to veterinarians for choosing which animals should be used for future studies, and what safeguards should be in place will be needed. This and other apprehensions were raised in another “Comment”, entitled “Part-revived pig brains raise slew of ethical quandaries” found in the same issue of Nature. In the study, there was no measurable EEG, and hence the conclusion that no consciousness or pain was being produced in the animals. It is important, however, to note that the EEG is the summation of the synchronized firing of multiple neurons within certain areas of the brain, and not a few or smaller groups firing. Does the perception of pain or minute levels of consciousness require EEG findings or does the firing of certain neurons and isolated activity at certain synapses in specific sub- areas accomplish the same? There is still so much that we don’t understand about the brain and the phenomenon of “perception” versus “awareness” and what constitutes consciousness. We are a long way from uttering the oft-quoted Dr. Frankenstein comment, “It’s alive!”, but this study starts to question some of our long-held beliefs about what constitutes death and when does irreversibility of biological function take place? Stay tuned for further studies in this area, but draw no conclusions yet! What is the issue with measles? The issue is that measles has not disappeared and in most parts of the world it accounts for many of the deaths of children- in India it is still one of the leading infectious disease causes of childhood deaths. Here in the U.S., we have become complacent about this vaccine preventable disease, and in the anti-vaccination community, more so. In the past, we have placed our faith upon the “herd immunity” concept in protecting us from communicable diseases. Herd immunity relies on the assumption that if a significant number of members of the community (or herd) have resistance to a disease (and that percentage varies according to the disease) then someone who doesn’t is protected by that “ring of immunity” around them (provided by the “herd”). So, if someone isn’t vaccinated, there is a strong likelihood they will have some degree of protection, since the disease they are at risk for won’t be circulating through the herd.
Well, in the age of rapid, world-wide travel – where the next pandemic could be an airline flight away- this just doesn’t hold true anymore. The percentage of a population needed to confer “herd immunity” for measles has been estimated at between 93-95%. This also assumes that things are stable within the herd. When we are dealing with a disease that is highly communicable (it has been estimated that one person with measles can infect 18 others!) it just doesn’t work in the age of world travel. If a person with no immunity goes to a country where there is a disease that is prevalent, or is there during an outbreak, then that person will contract the disease and/or bring it back to his/her community. If the immunity of the community, or the population that person circulates in, is less than 95% (this is the figure for measles protection), then there will be an outbreak. This is just what we have seen in the present outbreak in Brooklyn, where over 200 cases have occurred. Israel, (where, as I understand, there were recent visits by members of the affected Brooklyn community) has just gotten over an epidemic of measles (~3400) cases. According to the WHO, most were thought to have been brought in by tourists who were not immunized against the disease. So let’s take a quick look around the world: in the WHO Western Pacific Region in 2018 there were over 26,000 cases where the Philippines and China “led the pack”; in the WHO South and East Asian Region there were over 75,000 cases in 2018 where India clearly “led the pack” followed by Bangladesh; in the Americas in 2018, there were ~16,000 confirmed cases with Venezuela and Brazil “leading the pack”; and in the Who European region there were ~80,000 cases in 2018 with the Ukraine accounting for well over 30,000 of these. So, we are dealing with a disease that has not been eradicated, is highly contagious and, where in many parts of our own country, immunization rates among children have fallen below the required threshold to prevent its spread. Clearly, there is no surprise that we are in the midst of a measles outbreak in the U.S.- 314 cases in 15 different states, to date. This statistic is both depressing and appalling, because measles is so preventable; after one dose of MMR vaccine the efficacy is close to 93% and after the second dose it’s closer to 97%! We forget that measles is not without complications- 1 in 10 children will develop a severe ear infection because of measles; 1 in 20 people will develop a pneumonia; 1-2/1000 may die and 1/1000 may develop an encephalitis. So tragic, and so preventable. |